Today I’m presenting an interesting case of a mucinous ovarian neoplasm with an unusual tumor marker profile.
We had a 58-year-old postmenopausal female who presented with progressive abdominal distension and discomfort over a few months. There were no significant gastrointestinal symptoms such as altered bowel habits, bleeding per rectum, or weight loss.
On examination, a large abdominopelvic mass was palpable, extending above the umbilicus.
Tumor marker evaluation showed:
– CA 19-9: 108.2 U/mL (elevated)
– CA-125: within normal limits
– CEA: within normal limits
Given the elevated CA 19-9, we considered the possibility of a mucinous tumor, including a metastatic gastrointestinal origin. To rule this out, a colonoscopy was performed, which was completely normal.
The patient was taken up for staging laparotomy.
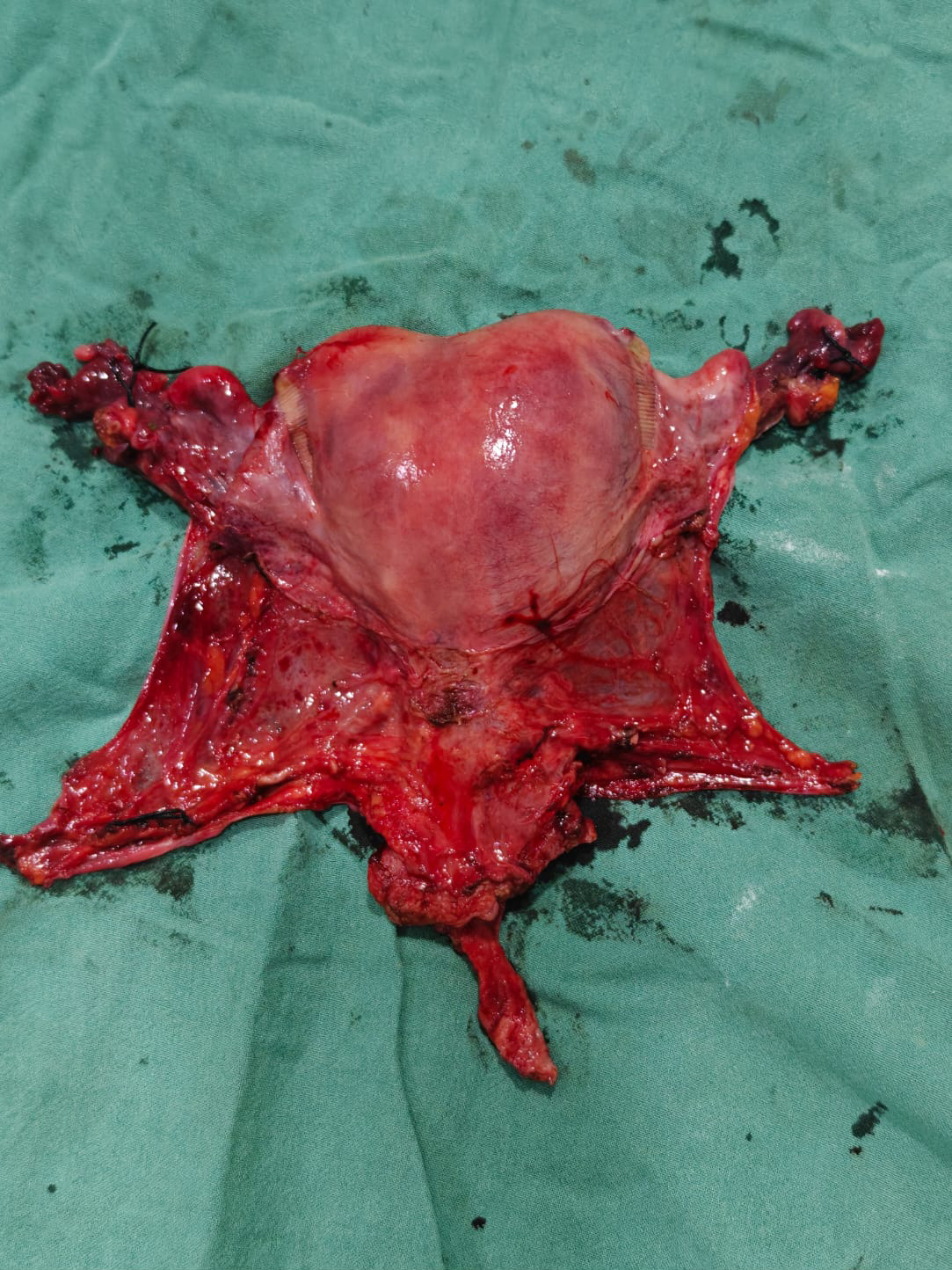
Intraoperatively, we found a large unilateral ovarian mass measuring approximately 22 × 20 cm. The surface was smooth, and there was no evidence of capsular breach or obvious peritoneal deposits.
We sent the specimen for frozen section, which suggested a mucinous ovarian neoplasm without clear invasive malignancy.
Based on these findings, we proceeded with comprehensive staging surgery, including:
– Total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH + BSO)
– Infracolic omentectomy
– Pelvic lymph node sampling
– Appendicectomy
– Peritoneal washings
There was no gross lymphadenopathy or peritoneal disease noted intraoperatively.
This case highlights a few important learning points:
First, mucinous ovarian tumors can present with markedly elevated CA 19-9, even when CA-125 and CEA are normal.
Second, ruling out a gastrointestinal primary is essential, especially in mucinous tumors, and colonoscopy plays a key role.
Third, large tumor size does not necessarily indicate malignancy in mucinous ovarian neoplasms.
Finally, comprehensive surgical staging remains the cornerstone of management in postmenopausal women.
Thank you.