Case Vlog
A 27-year-old woman presented with gradually increasing abdominal distension and mild pain. Ultrasound revealed a large multiloculated ovarian cyst. CT scan showed no metastasis. Tumor markers revealed normal CA-125 but elevated CA 19-9.
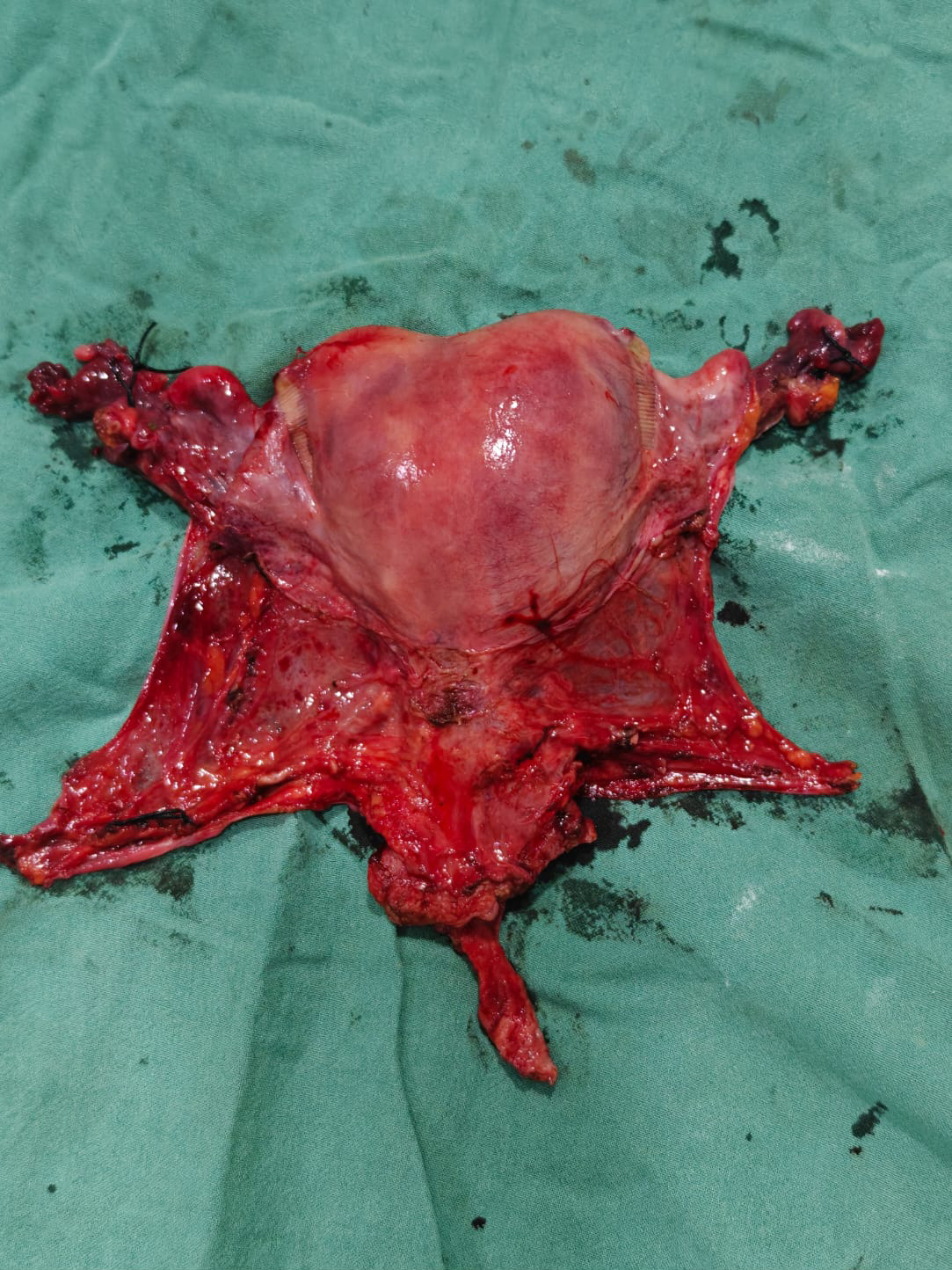
A staging laparotomy was performed. Intraoperatively, a large unilateral ovarian mass with smooth capsule and no peritoneal deposits was noted. Surgical staging including omentectomy and peritoneal biopsies was done.
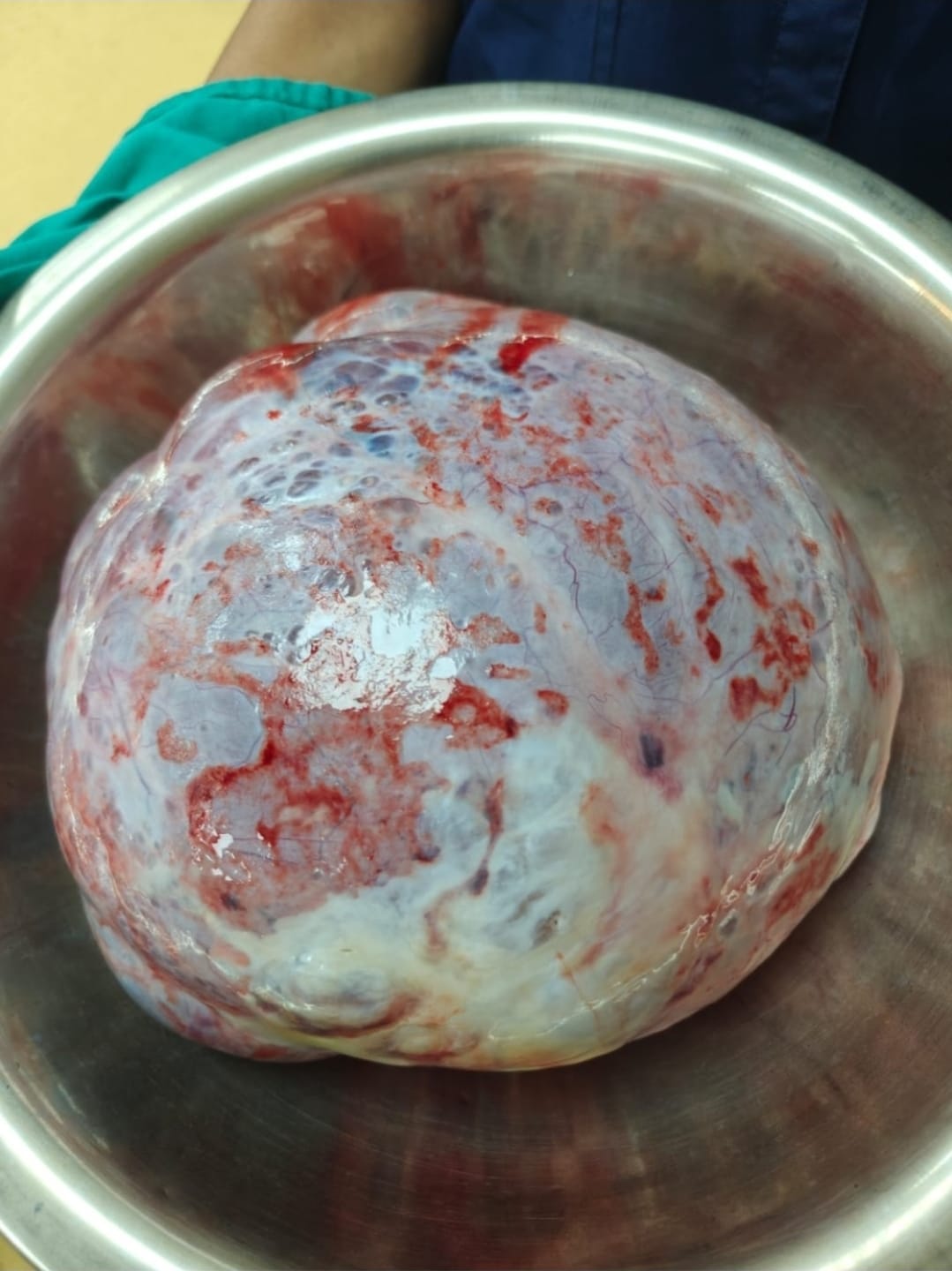
The specimen showed a large multiloculated cyst with mucinous content and focal hemorrhagic areas. Final histopathology confirmed mucinous carcinoma of the ovary.
This case highlights that normal CA-125 does not exclude malignancy, especially in mucinous ovarian tumors.
Discussion
Ovarian mucinous carcinoma is a rare subtype of epithelial ovarian cancer, accounting for approximately 3–5% of ovarian malignancies. It typically presents as a large unilateral cystic mass and often affects younger women.
Tumor markers play an important role in diagnosis. CA-125 may be normal or only mildly elevated, while CA 19-9 is frequently elevated, as seen in this case.
Differential diagnosis includes benign mucinous cystadenoma, borderline mucinous tumors, and metastatic mucinous tumors from the gastrointestinal tract. Distinguishing primary from metastatic tumors is crucial.
Primary tumors are usually large, unilateral, and have a smooth surface, whereas metastatic tumors are often bilateral, smaller, and show surface nodularity.
Management depends on staging. Early-stage disease is treated with surgical staging, and fertility-sparing surgery may be considered in young patients. Advanced disease requires cytoreductive surgery and chemotherapy, although mucinous tumors are relatively less responsive to standard platinum-based chemotherapy.
Prognosis is excellent in early-stage disease but poorer in advanced stages due to chemoresistance.