Borderline serous ovarian tumor is a distinct subtype of epithelial ovarian tumors characterized by epithelial proliferation, nuclear atypia, and complex papillary architecture without stromal invasion. It commonly affects women in reproductive or perimenopausal age groups and often presents as a cystic adnexal mass. Unlike invasive carcinoma, it demonstrates indolent behavior and excellent prognosis. Surgical management remains the cornerstone of treatment, ranging from fertility-sparing procedures to definitive surgery. Although recurrence can occur, especially with conservative surgery, overall survival is high, necessitating long-term surveillance .
Case Presentation:
A 38 year-old female homemaker from barasat presented with abdominal swelling for last 3 month.Usg showed one 10x 10 cm ovarian mass with ca 125 – 1183 and CT scan indicating possible ovarian neoplasm.
Management:
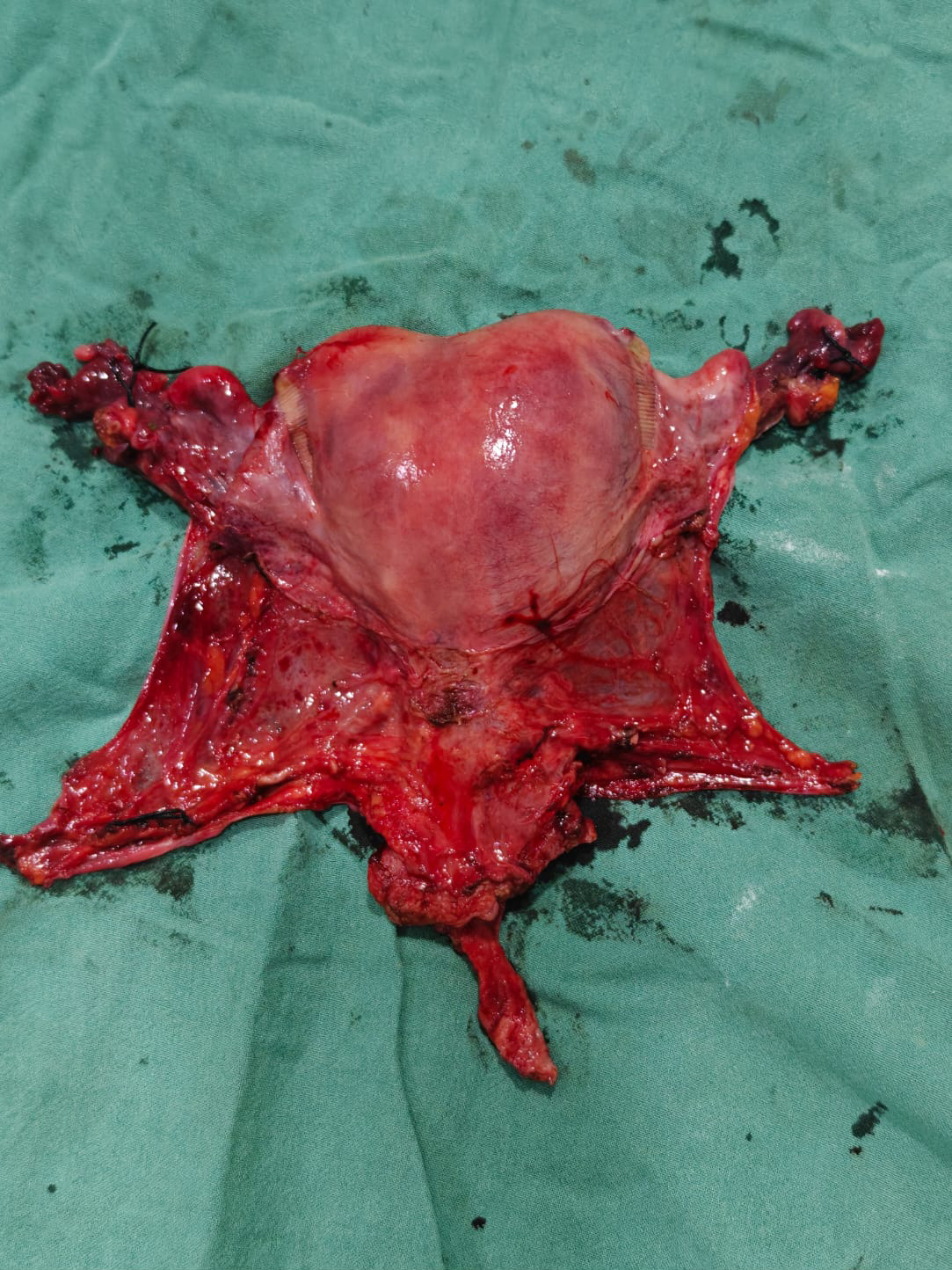
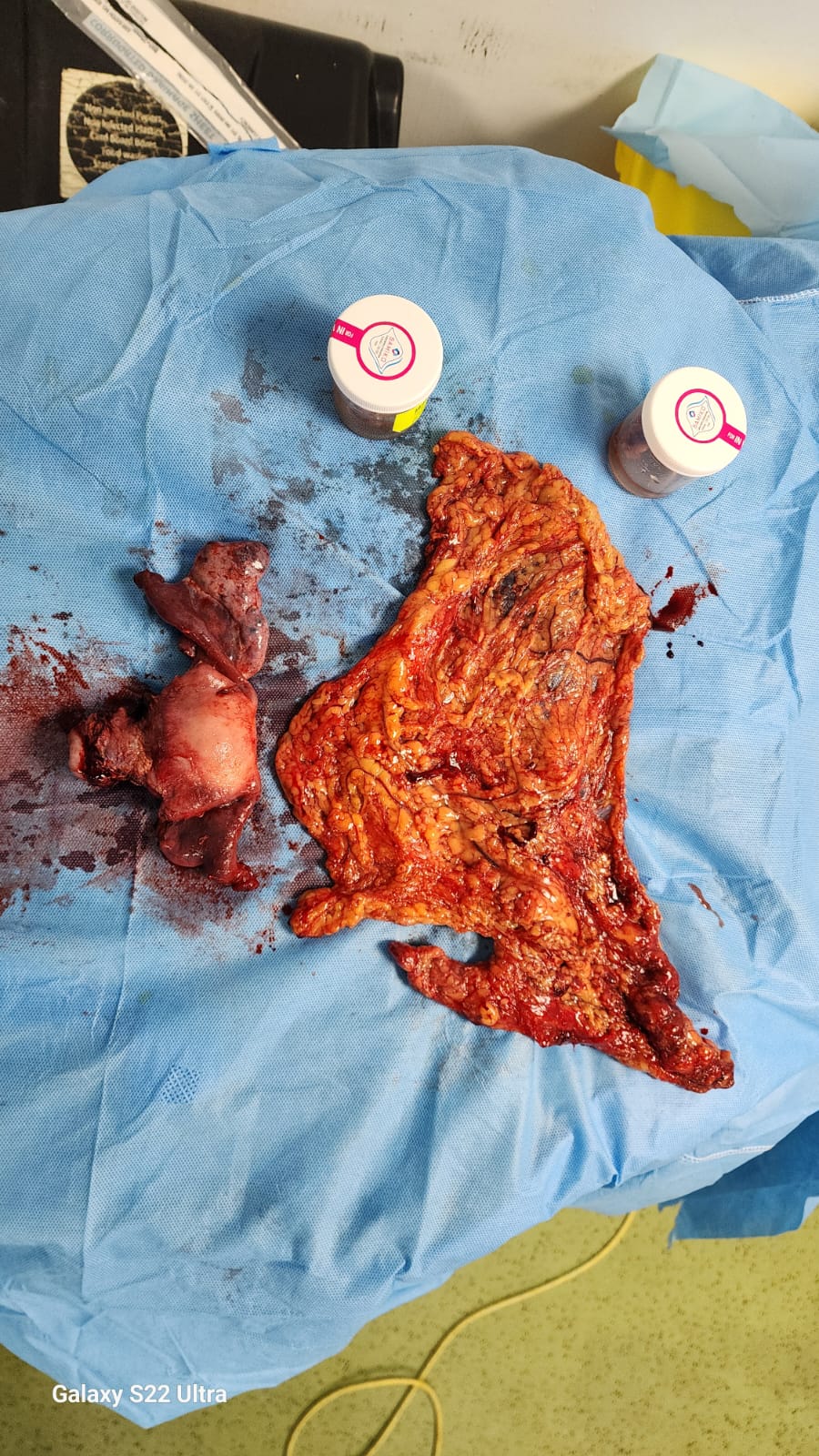
We planned for staging laparotomy with frozen section. Midline inciaion was made and the mass taken out in toto. Frozen report revealed it to be borderline tumor with microinvasion. We proceeded with complete staging which included TAH + BSO+ Infracolic omenetectomy + Pelvic and paraaortic node dissection. Pt recovered well and discharged on 5th day. IHC confirms the borderline tumor and patient is planned for only follow up
Conclusion:
Borderline serous ovarian tumor is an unique entity which requires surgical staging if microinvasion is suspected and close follow up. 5 year recurrece rate is below 1 %. No role of any adjuvant chemotherapy or radiotherapy.
Case Presentation:
A 38 year-old female homemaker from barasat presented with abdominal swelling for last 3 month.Usg showed one 10x 10 cm ovarian mass with ca 125 – 1183 and CT scan indicating possible ovarian neoplasm.
Management:
We planned for staging laparotomy with frozen section. Midline inciaion was made and the mass taken out in toto. Frozen report revealed it to be borderline tumor with microinvasion. We proceeded with complete staging which included TAH + BSO+ Infracolic omenetectomy + Pelvic and paraaortic node dissection. Pt recovered well and discharged on 5th day. IHC confirms the borderline tumor and patient is planned for only follow up
Conclusion:
Borderline serous ovarian tumor is an unique entity which requires surgical staging if microinvasion is suspected and close follow up. 5 year recurrece rate is below 1 %. No role of any adjuvant chemotherapy or radiotherapy.